Betsy Morris, a writer based in San Francisco, has a number of questions that serious people should answer before using (legitimately medicinal) experimental drugs. Her questions are from her article (from which this post’s title came) in Friday‘s Wall Street Journal. As a serious person (don‘t laugh so loudly), I have answers.
01 Should anybody be able to use experimental drugs before they have cleared clinical trials and gotten full FDA approval? Would your answer change if you knew that most clinical trials fail? How well-developed do you think a drug needs to be before it is available to everybody?
A Of course. 1) That’s the patient’s choice, ideally in consultation with his doctor, but not required except to the extent it’s the doctor who must obtain the drug and then administer it. It cannot be Government’s choice. Government’s sole role here is ensuring the patient has access to the drug’s risk profiles. 2) Why would it? See “risk profile.” 3) The drug needs to be FDA-certified safe. It’s efficacy, and whether a patient(s) wants to use it regardless of efficacy, is a market decision, not a Government one. Ideally, that certification would come from an objective, non-government entity; the FDA is too politicized. Unfortunately, we’re stuck with what we have.
02 Should somebody who is seriously ill have the same opportunity to take a promising but experimental drug if that drug is being made available to others? Would your answer change if you knew that it‘s the drug company that is deciding who gets to use it?
A Yes. 1) If a drug is available, it’s available. Full stop. 2) In today’s knee-jerk litigious society, “drug companies” need to protect themselves, and the only way they can is through patient selection. And that’s still weak protection.
03 Doctors frequently use FDA-approved drugs off-label, meaning for diseases or conditions for which the drugs haven‘t been tested or approved. Should the FDA allow this type of experimental but common drug use or should it be left to the judgment of the doctor?
A The FDA should have no input into off-label use beyond certifying the safety of the drug—which it already has done with its initial approval of the drug. After that, off-label use—and the efficacy of a drug—should be a market decision. Ideally, doctors would share (within HIPPA constraints) information about off-label uses and outcomes so a body of information can be built up regarding efficacy for this or that off-label use.
04 Instead of asking a drug company for an experimental drug, should a seriously or terminally ill patient be required to join a clinical trial? What if a patient in a trial has a good chance of getting a placebo?
A 1) No need to require the patient to enter a clinical trial. There’s no reason the drug company can’t ask the patient and his doctor to share associated data with the drug company, though; such data would be useful in fleshing out the formal clinical trial, so long as suitable statistical controls are applied to the extra-trial data. 2) The risk of getting a placebo is the risk everyone runs in a clinical trial, and if the patient is terminal, the risk is irrelevant. If the patient is seriously ill, he’s likely no worse off than any of the other seriously ill patients who are in the trial (were they not seriously ill, they would not be, for the most part, suitable trial candidates, anyway, especially in the early rounds of the trial).
05 Should patients be granted access to an experimental drug even if special access can make it harder to recruit enough people to conduct the clinical trials needed to determine whether the drug works and is safe? Does the benefit of a group of individual patients outweigh the potential future benefit to society of a treatment that has been fully vetted?
A Of course. 1) That’s the patient’s choice, ideally in consultation with his doctor, but not required except to the extent it’s the doctor who must obtain the drug and then administer it. It cannot be Government’s choice. Government’s sole role here is ensuring the patient has access to the drug’s risk profiles. Additionally, if the drug company is having trouble recruiting patients for a clinical trial, it should jump at this volunteering pool (however small) of patients. If the drug company isn’t having such trouble, a few extra-trial patients won’t interfere with anything. See above re extra-trial data collection. 2) The question is a non sequitur. Adding patients to the data collection process, even if from outside a clinical trial, can only enhance the overall data and analysis.
06 Do parents who have given informed consent to use an experimental drug on their terminally ill child give up their right to sue if the treatment backfires and kills the child prematurely? What if the parents were desperate, and unable to understand the poor odds of success?
A 1) Of course. They’re informed parents, they agreed to the risks and terms of participation a priori, and they have no right to change their minds after the fact. Otherwise, the agreements would be worthless, and drug companies would not allow an experimental drug to be used on a child, nor would they spend much effort or resource developing such drugs targeted for children. That’s the practical side. The moral side is that the parents signed the agreement and must honor their commitment. 2) Desperation has nothing to do with it. The parents are grown, rational human beings; especially with their children in tough situations, they need to act like grown rational human beings. The “unable to understand” bit is just a post hoc scare tactic.
07 Should a seriously or terminally ill child have an advocate separate from the parents and doctor when the decision is made to administer an experimental drug?
A Of course not. This is the parents’ decision, in consultation with the doctor, since it’s the doctor who must obtain and administer the drug. The only role—the only role—for a third party in this process is to facilitate the parents’ (and the child’s if he’s old enough/mentally mature enough to participate in the decision) understanding of the risk profile.
08 Is it all right to give an experimental drug to a terminally ill patient if the only reason to do so is to give the patient hope, even if there isn‘t any?
A Why would it not be? The only restriction would be if there is a limited supply of the drug, and it’s needed for the clinical trial(s). Besides, as a practical matter, the data collected, even from a terminally ill patient would be valuable: extend life, or not; improve the quality of remaining life, reduce the quality, have no effect; drug behave differently in terminally ill rather than merely seriously ill, but not yet terminal; ….
09 Often patients who get access to experimental drugs are those who are well-educated and savvy enough to know of clinical trials or experimental drug options. Should drugmakers be required to test experimental drugs across different demographic groups? What if the effort improves the efficacy of drugs among people of different groups, but slows drug development?
A 1) The question is just silly. Testing across (relevant) demographic groups is just good experimental technique; the educational or savviness of any particular group of patients is wholly irrelevant. To emphasize, though, the differing groups need to be relevant to the purpose of the drug. Shotgunning across groups, just because, would be a waste of resources. An experimental pregnancy management drug, for instance, need not be tested on a male demographic group of any sort. 2) The question is internally illogical. Testing across relevant demographic groups speeds development by obviating the need to repeat the test later across relevant but omitted groups. Apparently, Morris has missed the errors related to testing experimental drugs on white women while ignoring black women, and then trying to call the drug ipso facto good for black women, or testing experimental drugs on men, and then trying to call the drug ipso facto good for women.
10 Once an experimental drug gets the FDA‘s partial approval (called accelerated approval), a drugmaker is free to market the drug at almost any price. Are drug companies justified in charging whatever they can given the steep cost of drug development? What if paying for the drug will almost inevitably bankrupt the seriously ill person?
A I’ll elide the tacit cynicism that drug companies routinely charge almost any price on any of their drugs. 1) On what basis does anyone think a drug company will attempt to develop a drug if it’s not allowed to recoup the cost of development? The prices of experimental drugs, right along with the prices of established drugs, subsidize the cost of developing new drugs (and of producing established drugs). 2) How does that alter the economics of the matter? Further, the whole thrust of these 10 questions centers on whether a patient should have access to an experimental drug at all. Finally, if the drug is that expensive relative to a patient’s ability to pay—and it often (usually?) will be—that’s where charities, NGOs, and the like step in. A Government role? The taxpayers already are participating, outside of Government, through their donations to the charities, NGOs, and the like. There’s no need to double-tap them.

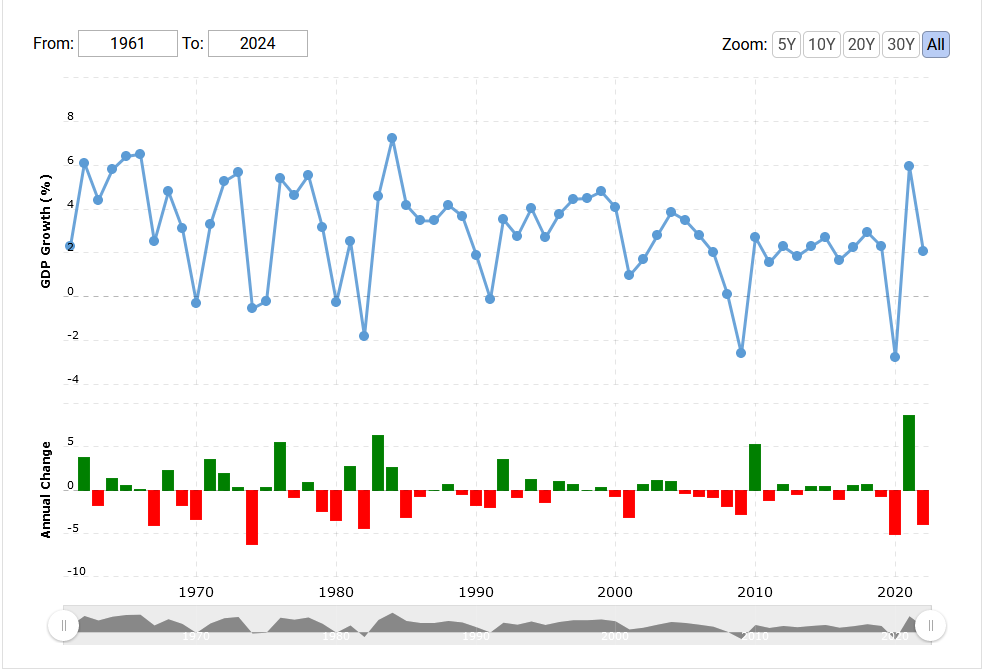
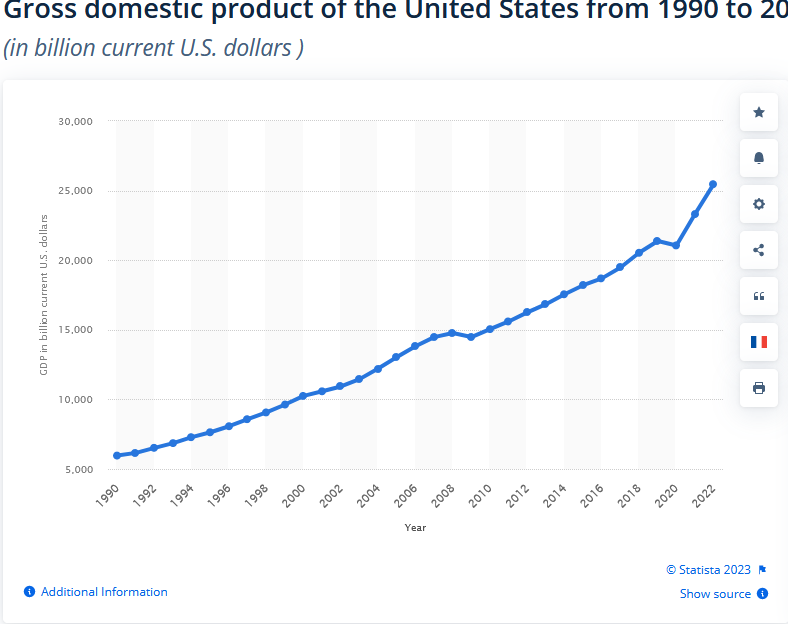 My challenge is this: find, in either graph, the Federal government shutdowns of 2013, 2018, and 2018-2019.
My challenge is this: find, in either graph, the Federal government shutdowns of 2013, 2018, and 2018-2019.